Mass psychogenic illness in nationwide in-school vaccination for pandemic influenza A(H1N1) 2009, Taiwan, November 2009 - January 2010
- Details
- Category: Vaccine Adverse Event Denialism
- Created: Wednesday, 08 September 2021 20:47
- Written by W T Huang , C C Hsu, P I Lee, J H Chuang
From 16 November 2009 to 22 January 2010, Taiwan investigated 23 clusters of mass psychogenic illness after vaccination (MPIV) in the nationwide in-school vaccination programme against the 2009 pandemic influenza A(H1N1). The median age of the 350 ill students (68% female) was 13 years. Intense media coverage of these events has driven public concerns about the safety of the pandemic influenza vaccine. In the future, countries should incorporate surveillance and communication strategies for MPIV in their pandemic preparedness plans.
The 2009 pandemic influenza A(H1N1) virus is highly transmissible in schools, and mathematical modelling suggests that vaccinating 70% of school children could mitigate a pandemic [1]. In Taiwan, schoolchildren (first to 12th grade) are among the priority groups to receive the pandemic influenza monovalent vaccine. On 16 November 2009, the government began a nationwide in-school influenza vaccination (NISIV) programme against pandemic influenza, using an inactivated vaccine without adjuvant (Adimmune Corporation, Taichung, Taiwan). Children under the age of nine years (first to third grade) received two doses, separated by approximately four weeks; children aged 10 years or older (fourth grade or higher) received one dose.
Mass adverse events following immunisation
On 23 November 2009, the government was notified that within two hours of pandemic influenza vaccination, a cluster of adverse events marked by dizziness, nausea and weakness occurred in 46 (7%) of the 692 schoolchildren aged 12 to 15 years who had received the vaccine at a middle school. Students were transported by ambulance to nearby hospitals and believed the illness was caused by the vaccine. Of the 46 ill students (26 female), physical and laboratory examinations found no organic cause for the reported symptoms. Forty-five patients recovered spontaneously and were discharged from the emergency department within 12 hours; one patient was hospitalised but discharged the following day. Public health officials reviewed the school vaccination process and found that all recommended procedures had been followed. It was concluded that this incident was a case of mass psychogenic illness after vaccination (MPIV) [2].
In response to safety concerns that might arise as the NISIV programme proceeded, we conducted enhanced surveillance to identify and investigate potential clusters of MPIV. Utilisation data on pandemic influenza vaccines were analysed to assess the impact of MPIV on vaccine coverage among schoolchildren.
Methods
Enhanced surveillance for mass psychogenic illness after vaccination
Each day, starting 23 November 2009, potential clusters of MPIV were retrospectively and prospectively identified through a search of two sources: (i) reports on adverse events following immunisation (AEFI) received by the national passive surveillance system jointly operated by the Taiwan Centers for Disease Control and the Taiwan Food and Drug Administration, and (ii) incident reports received by the Emergency Medical Management System, the Ministry of Health’s web-based system coordinating regional medical resources. A cluster of MPIV was defined as a constellation of symptoms suggestive of organic illness, but without an identifiable cause, in two or more children who were vaccinated on the same day, at the same school, and shared the belief that the pandemic influenza vaccine was the cause of the symptoms [3]. We requested that local health authorities provided additional details of illness onset, laboratory data, diagnoses, and treatment of ill students, and reviewed the storage and handling of the pandemic influenza vaccine involved in each cluster. The enhanced surveillance continued until 22 January 2010, the end of the school winter semester.
Monitoring pandemic influenza A(H1N1) monovalent vaccine coverage
The National Influenza Vaccine Information System (IVIS) receives daily electronic reports from all vaccination facilities on the pandemic influenza vaccine doses administered. Two measures of pandemic influenza vaccine coverage were calculated for schoolchildren from 16 November 2009 to 22 January 2010: (i) receipt of one or more doses for all students (dose 1), and (ii) receipt of two doses for students in first to third grade who had received the first dose (dose 2).
Results
Between 16 November 2009 and 22 January 2010, 23 clusters of MPIV in association with the NISIV programme were reported and investigated (Figure), including a total of 350 students. Each cluster involved between two and 46 ill students (median: 11). These clusters shared characteristics of the acute onset, the absence of physical or laboratory findings suggestive of an organic cause, the benign morbidity, the rapid spread and resolution of symptoms, and the absence of unprompted symptoms among students in other schools with exposures to the same batches of the vaccine. The age of the 350 ill students ranged from six to 16 years (median: 13), and 237 (68%) were female. Ten clusters involved 15 or more schoolchildren; the overall rate of illness among the 9,115 vaccinated students was 3% (range: 1–17%) (Table).
Figure. Cumulative percentage of schoolchildren receiving pandemic influenza A(H1N1) monovalent vaccine, by date of vaccination and dose received, Taiwan, 16 November 2009–22 January 2010
Table. Characteristics of mass psychogenic illness to pandemic influenza A(H1N1) vaccination involving 15 or more schoolchildren, Taiwan, 16 November 2009–22 January 2010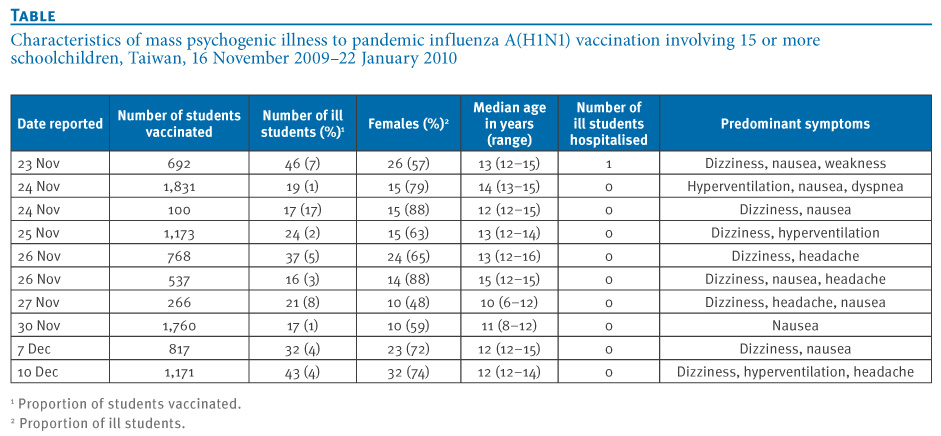
As of 22 January 2010, the cumulative percentage of schoolchildren receiving one or more doses of pandemic influenza vaccine was 75%; few schoolchildren received their first dose after mid-December 2009 (Figure). A total of 646,379 schoolchildren in first to third grade who received the first dose required a second dose, but only 313,144 (48%) did receive one by 22 January 2010.
Discussion
Although similar outbreaks of MPIV have been reported in school settings [2,4,5], to the best of our knowledge, this report is the first to describe that MPIV could occur as a result of mass introduction of vaccines to adolescents in a pandemic. Published literature suggests that, once vaccines are identified as a probable cause of mass psychogenic illness, a dismissive approach may actually be harmful [2]. In Taiwan, the government responded with rapidly investigating the school clusters of adverse events, well briefing the press, and reassuring the public with key messages that it was the process of vaccination, instead of the vaccine itself that triggered the occurrence of MPIV. On 1 December 2009, a guidance document was issued to school staff and local immunisation organisers regarding appropriate measures to minimise the risk of MPIV and prevent traumatic injuries related to fainting episodes after vaccination [6]. The recommendations included (i) vaccinating first those students who reported less fear of injections, (ii) providing a supportive group of volunteers or teachers to help relieve anxieties, and (iii) having students sitting down during the 30-minute observation period after vaccination. Through the aforementioned efforts, the number of MPIV reports decreased (four reports since 1 December 2009 compared with 19 reports from 16 to 30 November 2009), and we were able to proceed with the mass vaccination campaign against pandemic influenza.
This series of MPIV, along with the death of a first grade student on 21 December 2009 who died after receiving the vaccine, generated considerable media interest and had driven public concerns about the safety of the pandemic influenza vaccine in Taiwan. With a strengthened AEFI surveillance system, the government could rapidly detect and distinguish between true vaccine reactions, coincidental events, and injection reactions from the fear or pain of the injection itself rather than the vaccine [7,8]. However, not only were local health authorities unprepared to respond to possible outbreaks of MPIV in adolescents, but the requirement to vaccinate all students within two months limited the time available for education and consultation to healthcare providers and the public. Failure to communicate in advance that there are different causes of AEFI and a background of distrust of the domestically manufactured pandemic influenza vaccine provided the media with an opportunity to blame the vaccine for the mass adverse events. Although the government was able to reach a high vaccine coverage rapidly at the beginning, the subsequent stagnant progress on the first-dose vaccination and the low vaccine coverage for the second dose compared with the first dose coverage suggested a loss of confidence in the safety of the pandemic influenza vaccine, which undermined the impact of the NISIV programme in effectively achieving maximal coverage among schoolchildren.
In the future, public health officials should be aware that mass vaccination campaigns, particularly those targeting adolescents, could generate MPIV. Countries should incorporate surveillance and communication strategies for MPIV in their pandemic preparedness plans.
Acknowledgements
We thank the staff of local health authorities, Yu-Fang Tsai, Shi-Chuan Wang, Su-Ching Yao, Mei-Ling Wu, Yu-Yuan Hu, and Mei-Chu Lee for their support throughout the investigations.
References
- Yang Y, Sugimoto JD, Halloran ME, Basta NE, Chao DL, Matrajt L, et al. The transmissibility and control and pandemic influenza A (H1N1) virus. Science. 2009;326(5953):729–33.
- Clemens CJ. Mass psychogenic illness after vaccination. Drug Saf. 2003;26(9):599–604.
- Philen RM, Kilbourne EM, McKinley TW, Parrish RG. Mass sociogenic illness by proxy: parentally reported epidemic in an elementary school. Lancet. 1989;2(8676):1372–6.
- Khiem HB, Huan le D, Phuong NT, Dang DH, Hoang DH, Phuong le T, et al. Mass psychogenic illness following oral cholera immunization in Ca Mau City, Vietnam. Vaccine. 2003;21(31):4527–31.
- Buttery JP, Madin S, Crawford NW, Elia S, La Vincente S, Hanieh S, et al. Mass psychogenic response to human papillomavirus vaccination. Med J Aust. 2008;189(5):261–2.
- Centers for Disease Control and Prevention (CDC). Syncope after vaccination — United States, January 2005–July 2007. MMWR Morb Mortal Wkly Rep. 2008;57(17):457–60.
- Immunization safety surveillance: guidelines for managers of immunization programmes on reporting and investigating adverse events following immunization. Manila: World Health Organization Western Pacific Regional Office; 1999. Report No. WPRO/EPI/99.01. [Accessed 20 May 2010]. Available from: http://www.who.int/immunization_safety/publications/aefi/en/AEFI_WPRO.pdf.)
- Huang WT, Chuang JH, Kuo SH. Monitoring the safety of pandemic H1N1 vaccine. Lancet. 2010;375(9721):1164.
Source: https://www.eurosurveillance.org/content/10.2807/ese.15.21.19575-en and https://pubmed.ncbi.nlm.nih.gov/12814329/
